If you’ve been dealing with knee pain for years and your doctor just said it’s time for surgery, you probably have one big question running through your head: which knee replacement is best for me? It’s a fair question, and honestly, it deserves a thorough answer rather than a quick five-minute explanation in a busy clinic.
This guide breaks down the different types of knee replacements, which implant is best for knee replacement based on your situation, and which is the best material for knee replacement currently available. Whether you’re 55 and active or 72 and just want to walk without pain, this should help you have a much better conversation with your surgeon.
What Actually Happens During a Knee Replacement?
Before getting into which knee replacement is best, it helps to understand what surgeons are actually doing. A knee replacement removes the damaged cartilage and bone surfaces of your knee and replaces them with artificial components, called an implant or prosthesis. These components recreate the smooth gliding surface that your natural knee cartilage used to provide.
The procedure has been around since the 1970s and has improved steadily since then. Today, more than 700,000 knee replacement surgeries are performed each year in the United States alone, and satisfaction rates are generally high when patients are properly selected and the right implant is chosen.
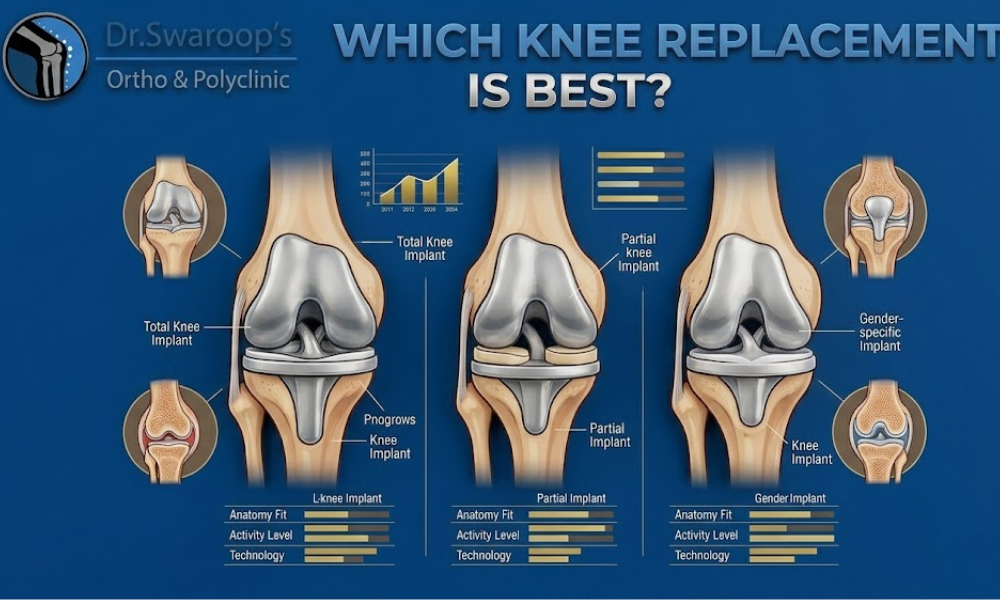
Types of Knee Replacement: Which One Suits You?
Not all knee replacements are the same. The type your surgeon recommends depends on how much of your knee is damaged, your age, activity level, and overall health.
Total Knee Replacement (TKR)
Total knee replacement is the most common procedure. It replaces all three compartments of the knee, the medial (inner), lateral (outer), and patellofemoral (kneecap) compartments. If your arthritis is widespread across the entire knee, this is almost always the recommended route.
TKR implants typically last 15 to 20 years, sometimes longer with proper care. Studies show that around 90% of total knee replacements are still functioning well at the 10-year mark, which is reassuring for most patients.
Partial (Unicompartmental) Knee Replacement
If only one compartment of your knee is affected, a partial knee replacement might be an option. Because it preserves more of your natural bone and tissue, recovery tends to be faster and the knee often feels more natural afterward.
However, not everyone qualifies. You need to have intact ligaments, a healthy weight range, and damage limited to one compartment. If there’s any chance the arthritis will spread to other parts of the knee, a total replacement might make more long-term sense.
Patellofemoral Replacement
This is a less common type that targets only the kneecap compartment. It’s typically recommended for people who have isolated kneecap arthritis without involvement of the rest of the joint. It’s not widely performed because patient selection has to be very precise for it to work well.
Bilateral Knee Replacement
Some patients need both knees replaced. This can be done simultaneously (both at once) or staged (one knee at a time). Most surgeons prefer the staged approach because it reduces surgical risk and makes rehabilitation easier to manage.
Which Implant Is Best for Knee Replacement?
This is where things get a bit more specific. The implant design affects how your knee moves, how long it lasts, and whether you’ll have restrictions on activity afterward.
Fixed-Bearing vs. Mobile-Bearing Implants
In a fixed-bearing implant, the plastic (polyethylene) insert between the metal components doesn’t move. It’s the most commonly used design worldwide and has decades of proven performance behind it.
In a mobile-bearing implant, that plastic insert can rotate slightly. The idea is that this rotation reduces wear over time. Some studies support better long-term wear characteristics with mobile-bearing designs, but the clinical differences aren’t dramatic for most patients, and mobile-bearing implants require more precise surgical technique to perform well.
For the average patient, a well-placed fixed-bearing implant performs excellently and is a lower-risk choice.
Posterior-Stabilized vs. Cruciate-Retaining Implants
Your knee has ligaments called the anterior and posterior cruciate ligaments (ACL and PCL). During knee replacement, the ACL is always removed. What happens to the PCL depends on the implant type.
Cruciate-retaining (CR) implants preserve the PCL, which some surgeons feel gives a more natural feel to the knee. Posterior-stabilized (PS) implants remove the PCL and use a post-and-cam mechanism in the implant to compensate.
Neither is universally better. Some surgeons prefer CR for younger, active patients. Others default to PS because it’s technically more forgiving. It largely comes down to your surgeon’s preference and your knee’s anatomy.
Gender-Specific Implants
Some manufacturers offer implants designed with the anatomical differences between male and female knees in mind, particularly the narrower femur width common in women. Research on whether gender-specific implants produce better outcomes is mixed. Some studies show modest improvement in patient satisfaction; others find no significant difference. If your surgeon offers this option, it’s worth discussing.
High-Flex Implants
Standard implants typically allow flexion up to around 120 degrees, which is adequate for most daily activities. High-flex designs are engineered to allow up to 155 degrees of flexion, which can be important for patients who need to kneel for religious practices or cultural reasons.
Which Is the Best Material for Knee Replacement?
Material science plays a big role in how long your knee implant will last and how it performs under load. Understanding which is the best material for knee replacement helps you ask your surgeon the right questions.
Metal Components: Cobalt-Chromium vs. Titanium
The femoral (thigh bone) component and tibial tray (shin bone base) are typically made from metal. Two materials dominate:
Cobalt-chromium alloy is the gold standard for the femoral component. It’s extremely hard and polishes to a very smooth surface, which reduces wear on the plastic insert beneath it. Cobalt-chromium has a long track record going back decades.
Titanium alloy is more commonly used for the tibial tray and sometimes for cementless implants because it bonds exceptionally well with bone. Titanium is also the better choice for patients with a known nickel sensitivity, since cobalt-chromium contains some nickel.
Some newer implants use oxidized zirconium, a material that combines a zirconium metal core with a hard ceramic-like surface. Studies suggest oxidized zirconium can reduce plastic wear by up to 85% compared to cobalt-chromium. It may be a good fit for younger, more active patients who want maximum longevity from their implant.
The Plastic Insert: Polyethylene Quality Matters
Between the metal components sits a polyethylene (plastic) bearing surface. This is the part that absorbs shock and allows smooth movement, and it’s also the part most likely to wear out over time.
Standard polyethylene has largely been replaced by highly cross-linked polyethylene (HXLPE), which is treated to create stronger molecular bonds. HXLPE is significantly more wear-resistant than conventional plastic and has become the standard in most modern implants.
Vitamin E-stabilized polyethylene takes this a step further by incorporating vitamin E (tocopherol) into the plastic to prevent oxidation over time. This matters because oxidation weakens polyethylene after years of use. For patients expected to live 20 or more years with their implant, vitamin E-stabilized plastic is worth asking about.
Cementless vs. Cemented Fixation
How the implant attaches to your bone is another material-related decision.
Cemented fixation uses surgical bone cement (acrylic) to bond the implant to your bone. It provides immediate, strong fixation and has a long history of success. For older patients or those with softer bone, cemented implants remain the most reliable option.
Cementless fixation uses implants with a porous surface coating that allows your bone to grow directly into the implant over time. It’s increasingly popular for younger, more active patients because there’s no cement layer that can eventually loosen. However, it requires good bone quality for the bone ingrowth to succeed properly.
Some surgeons use a hybrid approach: a cemented tibial component (which takes more force) with a cementless femoral component.
Robotic and Computer-Assisted Knee Replacement
One factor that deserves mention when discussing which knee replacement is best is how it’s performed, not just what implant is used.
Robotic-assisted knee replacement systems like Mako (Stryker) have become increasingly available. These systems use CT scan data to build a 3D model of your knee before surgery, allowing your surgeon to plan component placement precisely. During surgery, the robotic arm helps the surgeon stay within the planned boundaries.
Early data suggests robotic-assisted surgery improves implant alignment accuracy. Better alignment means less uneven wear and potentially longer implant life. Some studies also show faster recovery and better early outcomes. Whether these advantages translate into meaningfully better 15 or 20-year survival rates is still being established, but it’s a promising development.
How Long Will a Knee Replacement Last?
Most patients ask this before anything else. The honest answer is: it depends on several factors including your age, weight, activity level, the implant design, and the quality of surgical technique.
For a typical patient in their late 60s or early 70s, a well-placed knee replacement using modern implant materials has a realistic expectation of 20 or more years. For a 55-year-old who’s very active, revision surgery within 15 to 20 years is a possibility worth planning for.
Obesity is one of the strongest risk factors for early implant failure because the increased load accelerates wear. Losing even modest weight before surgery can make a meaningful difference in how long your implant lasts.
Questions to Ask Your Surgeon Before You Decide
Once you understand the basics of which knee replacement is best, you’re in a much better position to have an informed conversation. Here are some questions worth bringing to your appointment:
- Which type of implant do you typically use, and why?
- Are you using cross-linked or vitamin E-stabilized polyethylene?
- Is the implant cemented, cementless, or hybrid, and why is that right for me?
- Do you offer robotic-assisted surgery, and am I a good candidate?
- How many knee replacements do you perform per year?
That last question matters more than most people realize. Surgeon volume is consistently linked to better outcomes. High-volume surgeons tend to have fewer complications and better long-term results.
Frequently Asked Questions
Q: Which knee replacement is best for younger patients under 60? Younger patients generally benefit from cementless fixation (to allow bone ingrowth), highly wear-resistant polyethylene (HXLPE or vitamin E-stabilized), and oxidized zirconium femoral components when available. Robotic-assisted placement also makes sense to maximize implant alignment for the long term.
Q: Which implant is best for knee replacement in active patients? For active patients who want to return to sports like cycling, swimming, or hiking, a high-flex design combined with durable materials like oxidized zirconium and cross-linked polyethylene tends to perform well. Discuss your specific activity goals with your surgeon so the implant choice reflects your lifestyle.
Q: Which is the best material for knee replacement in patients with metal allergies? Patients with nickel sensitivity or confirmed metal allergies should discuss oxidized zirconium or titanium-based implants. These avoid the nickel content found in cobalt-chromium alloys. Patch testing before surgery can help confirm which metals are problematic.
Q: How do I know if I need a total or partial knee replacement? Your surgeon will base this on X-rays, MRI scans, and a physical examination. If arthritis is confined to one compartment and your ligaments are intact, partial replacement is a possibility. Most patients with widespread arthritis will need a total replacement.
Q: Is robotic knee replacement better than traditional surgery? Robotic-assisted surgery improves the precision of implant placement, which is linked to better long-term outcomes. It doesn’t change the implant itself, but it does reduce the chance of malalignment. For most patients, it’s worth choosing a surgeon who offers this technology if it’s accessible.
Q: What activities should I avoid after knee replacement? High-impact activities like running, jumping, and contact sports are typically discouraged because they accelerate implant wear. Walking, cycling, swimming, and golf are generally well-tolerated. Your surgeon will give you specific guidance based on your implant type and overall health.
Q: How long is recovery after knee replacement surgery? Most patients walk with assistance within 24 hours of surgery. By 6 weeks, many can manage daily activities independently. Full recovery, where you feel like yourself again, typically takes 3 to 6 months. Physical therapy plays a large role in how quickly and completely you recover.
Final Thoughts
There’s no single answer to which knee replacement is best, because the right choice genuinely depends on your age, activity level, anatomy, and long-term goals. But by understanding the differences between implant types, materials, and surgical techniques, you’re no longer walking into that surgeon’s office without a clue.
The general direction research points toward: modern cementless or hybrid fixation for younger patients, highly cross-linked or vitamin E-stabilized polyethylene for durability, oxidized zirconium for those wanting the lowest possible wear rate, and robotic-assisted surgery when available for better precision. For older patients or those with softer bone, cemented implants remain excellent, proven options.
Have an honest conversation with your surgeon about your lifestyle goals, not just your pain level. The best knee replacement is the one placed correctly, with appropriate materials, by a surgeon who does this regularly. That combination gives you the best shot at an active, comfortable life for the next 20 years and beyond.
Dr. Swaroop Solunke
Dr. Swaroop Solunke is one of the very few orthopedic surgeons in Pune who has trained across three continents specifically in joint replacement surgery. He completed his MBBS from Dr. D.Y. Patil University, Navi Mumbai (2009), followed by his MS in Orthopaedics from MGM Medical College, Kamothe (2014), graduating as a gold medalist from one of the Mumbai region’s busiest trauma units.
His post-graduation training took him to Germany for a fellowship in arthroplasty at Bruderkrankenhaus St. Josef Hospital, Paderborn, and then to Milan, Italy, where he trained in primary and revision hip replacement under Dr. Luigi Zagra at IRCCS Instituto Ortopedia Galeazzi. He later completed an advanced fellowship in robotic knee replacement at the Stone Research Foundation in San Francisco, California, making him part of a small group of US-trained robotic knee surgeons currently practicing in Pune.
With over 16 years of overall medical experience and 11 years as a dedicated orthopedic and joint replacement specialist, Dr. Solunke practices at Dr. Swaroop’s Ortho and Polyclinic in Wakad, PCMC. His approach is straightforward: surgery is the last option, not the first recommendation. Around 60% of patients who consult him concerned about a knee replacement leave with physiotherapy and medication instead.
He performs every surgery personally and consults in Marathi, Hindi, and English, whichever language the patient and family are most comfortable with.
Qualifications at a Glance:
- MS Orthopaedics, Gold Medalist, MGM Medical College
- MBBS, Dr. D.Y. Patil University, Navi Mumbai
- Fellowship in Arthroplasty, St. Josef Hospital, Paderborn, Germany
- Fellowship in Hip Replacement, IRCCS Instituto Ortopedia Galeazzi, Milan, Italy
- Fellowship in Robotic Knee Replacement, Stone Research Foundation, San Francisco, USA
- Member, Indian Medical Association (IMA)
- Member, Indian Orthopaedic Association (IOA)
- Member, Maharashtra Orthopaedic Association
- Member, Pune Orthopedic Society
Clinic Locations: Wakad (primary OPD), Kush Neuro Cardiac Hospital Wakad (surgical cases), Joint Aura Ortho and Polyclinic, Nigdi-Pradhikaran
Book an Appointment with Dr. Swaroop Solunke
If knee pain has been slowing you down and you want an honest, expert opinion on whether replacement surgery is right for you, Dr. Solunke’s clinic is open seven days a week.
Dr. Swaroop’s Ortho and Polyclinic Shop No. 304, Sonigara Kesar, Near PNB Bank, Chhatrapati Chowk, Wakad, Pune, Maharashtra 411057
Phone: +91 73854 86860
Email: dr.swaroopsolunke@gmail.com
WhatsApp Appointment: Click here to book on WhatsApp
Online Appointment: Book at orthopedicclinicinpcmc.com
Open Monday to Sunday, 24 hours for emergencies.

Dr. Swaroop Solunke
- Fellowship in Arthroplasty (Germany)- Bruderkrankenhaus St. Josef Paderborn, Germany.
- Fellowship in Primary and Revision Hip Replacement – Dr. Luigi Zagra IRCCS Instituto Orthopedia Galeazzi, Milan, Italy.
- Fellowship in Arthroplasty (Germany)- Bruderkrankenhaus St. Josef Paderborn, Germany.
- Fellowship in Robotic Knee Replacement – The Stone Research Foundation, San Francisco, California, USA.
- MS - Orthopaedics (Gold Medalist) – MGM Medical College and Hospital.
- MBBS – Dr. DY Patil University, Navi Mumbai.
- Member of Indian Medical Association (IMA)